
From the 1Department of Community Medicine and Rehabilitation, Rehabilitation Medicine, Umeå University, Umeå, 2Pain and Rehabilitation Centre and, Department of Medical and Health Sciences, Faculty of Medical and Health Sciences, 3Department of Medical and Health Sciences, Physiotherapy and 4Department of Behavioural Sciences and Learning, Linköping University, Linköping, Sweden
Objectives: To investigate the outcomes one year after multimodal rehabilitation programmes in primary care for patients with chronic pain, both as a whole and for men and women separately. A second aim was to identify predictive factors for not being on sickness absence at follow-up after one year.
Methods: A prospective longitudinal cohort study of 234 patients, 34 men and 200 women, age range 18–65 years, who participated in multimodal rehabilitation programmes in primary care in 2 Swedish county councils. Pain, physical and emotional functioning, coping, health-related quality of life, work-related factors, sickness absence (sick leave, sickness compensation/disability pension) were evaluated prior to and one year after multimodal rehabilitation programmes.
Results: Patients showed significant improvements at 1-year follow-up for all measures (all p ≤ 0.004) except satisfaction with vocation (p = 0.060). The proportion of patients on sick leave decreased significantly at follow-up (p = 0.027), while there was no significant difference regarding the proportion of patients on sickness compensation/disability pension (p = 0.087). Higher self-rated work ability was associated with not being on sickness absence at 1-year follow-up (odds ratio (OR) 1.19, 95% confidence interval (CI) 1.21–1.06, p = 0.005).
Conclusion: This study indicates that multimodal rehabilitation programmes in primary care could be beneficial for patients with chronic pain, since the outcomes at 1-year follow-up for pain, physical and emotional functioning, coping, and health-related quality of life were positive. However, the effect sizes were small and thus further development of multimodal rehabilitation programmes is warranted in order to improve the outcomes.
Key words: multidisciplinary; rehabilitation; pain; primary care; outcome; sex.
Accepted Jan 16, 2020; Epub ahead of print Jan 29, 2020
J Rehabil Med 2020; 52: jrm00023
Correspondence address: Elisabeth Pietilä-Holmner, Department of Community Medicine and Rehabilitation, Rehabilitation Medicine, Umeå University, SE-901-87 Umeå, Sweden. E-mail: elisabeth.pietila.holmner@umu.se
For patients with chronic pain, studies have shown that multimodal rehabilitation programmes at specialist care level have positive effects. Since there is limited knowledge about the long-term effects of multimodal rehabilitation programmes in a primary care setting this study investigated the effects of multimodal rehabilitation programmes in 234 patients with chronic pain, 34 men and 200 women, age range 18–65 years, who participated in multimodal rehabilitation programmes in primary care in 2 Swedish county councils. At 1-year follow-up patients reported small improvements in pain, physical and emotional functioning, coping, and health-related quality of life. The proportion of patients on sick leave decreased, while there was no difference regarding the proportion of patients on sickness compensation/disability pension. This study indicates that multimodal rehabilitation programmes in primary care could be beneficial for patients with chronic pain.
Chronic pain, defined as pain lasting more than 3 months, is a common disorder which has far-reaching consequences both for the individual and society (1). Chronic pain conditions are influenced by physical, psychological, emotional and social factors, and affect several aspects of life and everyday functions, both during leisure and working time (1). For society, chronic pain often gives rise to large economic costs due to long-term sick leave, high utilization of healthcare resources, and lost productivity (2). Chronic pain conditions are complex, and approximately 20% of the Swedish population reports chronic pain with moderate to severe intensity, the majority consisting of musculoskeletal pain (1, 3). Surveys have shown that 20–40% of primary care visits are related to pain, and approximately half of those are due to some form of chronic pain (4).
For patients with chronic pain, several studies have shown that multimodal rehabilitation programmes (MMRPs) have more positive effects on perceived pain, activity, function, and return to work, compared with unimodal rehabilitation (1, 3, 5). According to the International Association for the Study of Pain (IASP)’s definition of MMRP as a part of interdisciplinary treatment (6), MMRP is provided by a multidisciplinary team that collaborates in assessment and treatment based on the bio-psycho-social model of chronic pain (1, 7) and that share common goals. The core goals of rehabilitation programmes in general, and especially for patients with chronic pain, are broad and multifactorial (e.g. reduced psychological distress, reduced pain intensity, better coping strategies, return to work/studies and increased health-related quality of life (HRQoL)) in combination with individualized goals of the patient. An important prerequisite for MMRP is that the patient is an active participant in fruitful collaboration with the team to achieve the individual rehabilitation goals (1).
Women have a somewhat higher prevalence of chronic pain and longer pain duration than men (8). Some studies have indicated that men and women may benefit unequally from MMRP regarding pain and activity in daily life (9), but there is still a lack of knowledge regarding sex-related differences on the effects of MMRP.
MMRP has a long tradition in pain rehabilitation at specialist care level for patients with severe complex chronic pain, but after the Swedish rehabilitation guarantee was introduced in 2009, MMRPs were also applied in primary healthcare for patients with less complexity of the chronic pain condition regarding psychological factors. A criterion was that patients should have tried unimodal rehabilitation, e.g. pharmacological treatment or physiotherapy, before participating in MMRP, without reaching any noticeable effects. The rehabilitation guarantee was an initiative by the government to reduce sickness absence. National guidelines were published to support assessment of patients with chronic pain; they offered selection criteria to enhance MMRP at the appropriate level (specialist vs primary healthcare) (10).
In Sweden working age for most persons is 18–65 years, but it is possible for an individual to retire from the age of 61–68 years. Depending on work capacity, sick leave and sickness compensation/disability pension could be obtained for full-time (100%) or part-time (25–75%). There is a time-frame of a maximum of 364 days during a 450-day period for sickness benefits (80% of work income). If work capacity remains reduced after that time, extended sickness benefit (75% of work income) can be applied for up to 550 days. Furthermore, persons with severe illness can be granted sickness benefits, and persons with long-term disease who will probably never be able to work can obtain sickness compensation/disability pension (11).
The rehabilitation guarantee ensured that healthcare providers received special financial compensation for patients with non-specific chronic pain who completed MMRP. However, there is limited knowledge on the long-term effects of MMRP in a primary care setting for patients with chronic pain. Moreover, knowledge is lacking regarding factors that could be associated with the ability to work after MMRP. If modifiable factors can be identified, they could be targeted during the MMRP. Therefore, we conducted a longitudinal study of patients with chronic pain participating in MMRP in primary care in 2 Swedish county councils.
Hence, the primary aim of this study was to investigate the long-term outcomes, including effect sizes (ES), of MMRP in primary care on pain, physical and emotional functioning, HRQoL and work-related factors for a group of patients with chronic pain, both as a whole and for men and women separately. A second aim was to identify predictive factors for not being on sickness absence at 1-year follow-up.
Design
This prospective longitudinal cohort study, with 1-year follow-up, investigated patients with musculoskeletal chronic pain who participated in MMRP in primary care.
Setting
The study was carried out in 2 Swedish county councils: one in northern Sweden (Västerbotten), the other in southern Sweden (Östergötland). All patients, at 5 primary care centres in northern Sweden and at 6 in southern Sweden, who participated in MMRP between 29 August 2012 and 16 December 2015 were invited to participate in the study.
Before participating in MMRP, each patient was assessed, selected and referred for MMRP by a physician or a team in primary care. According to Swedish guidelines there is a medical indication for MMRP in primary care if the patient has chronic pain that significantly limits the patient’s daily life, and if the patient has the potential to improve despite the pain .The patient should also have tried unimodal treatment, e.g. pharmacological treatment or physiotherapy, without reaching any noticeable effects (10). The degree of negative psychological components (depression, anxiety and fear avoidance), prevalence of co-morbidity that can affect the pain and its consequences, as well as pain intensity, determine whether the patient should be treated in specialist vs primary healthcare. Patients with moderate degree of complexity, i.e. low degree of negative psychological components, no co-morbidity, as well as moderately high pain intensity, should be recommended MMRP in primary care, while patients with high degree of psychological components and high pain intensity should be recommended MMRP in specialized care.
Inclusion criteria for MMRP were: age range 18–65 years, disabling chronic pain, potential for an active life change, and no other diseases or conditions that precluded participation in MMRP. Patients needed to be either on sick leave or experiencing major interference in everyday life due to chronic pain and thus at risk of sick leave.
The MMRP was based on a bio-psycho-social approach with interdisciplinary teamwork and included goalsetting together with the patient and interventions, such as physical exercise, relaxation, training in coping strategies based on cognitive behavioural therapy (CBT), and education in pain management. The MMRP lasted 6–10 weeks, 1.5–3.5 h/week, was conducted as a group intervention, or as a combination of a group intervention and individual sessions. MMRP teams consisted of different professionals in different teams, but involved at least a physiotherapist and occupational therapist. In each team, general practitioners, social workers or psychologists were either part of the team or had a consulting role. The general practitioners also had medical responsibility for the patients. All teams were trained in interdisciplinary approaches by teams from specialist care.
Ethical approval
The study was approved by the Regional Ethical Review Board in Umeå, Sweden (Dnr: 2013-192-31 M) and was conducted in accordance with the STROBE guidelines for cohort studies. All participants signed a written informed consent form prior to enrolment. Participants were free to omit any items in the questionnaires or withdraw from the study at any time without providing an explanation. The study was performed in accordance with the principles of the Declaration of Helsinki.
Procedure
All patients completed the questionnaires on 3 occasions: before the assessment, at the end of MMRP and at 1-year follow-up. At the 1-year follow-up, the questionnaire was sent home to be returned by post in a prepaid addressed envelope. A reminder was sent to the patient if no answer was received within 4 weeks.
Assessment/questionnaires
Since 1998, the effects of multimodal rehabilitation at specialist clinics have been continuously evaluated in the Swedish Quality Registry for Pain Rehabilitation (SQRP) (12). To evaluate MMRP in primary care, the research group prepared comprehensive questionnaires with patient-reported outcome measurements (PROMs), combining standardized instruments from the SQRP for specialist care with some additional variables to adapt the questionnaires to primary care conditions. The questionnaire included demographics and questions regarding pain duration, number of pain sites and pain intensity as well as education, country of birth, work situation, sick leave and prognosis of return to work. Most of the included instruments covered the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT) core outcome domains for the treatment of patients with chronic pain (13) and validation and application of a patient-relevant core set of outcome domains to assess multimodal pain therapy (VAPAIN)(14). In this study, data at the start of the study and at 1-year follow-up were used. The investigated areas in the present study were sociodemographic, pain, emotional and physical functioning, coping, health, and work-related factors.
Sociodemographic data
Age (years) and sex.
Country of birth was reported in 4 categories (Sweden, Nordic country outside Sweden, European but non-Nordic country, or non-European country) and recoded into 3 categories (Swedish, European, or non-European).
Level of education was reported on 4 levels (compulsory school, upper secondary/vocational school, university/college, or other) and used as a 3-level variable after re-coding “other” as missing (compulsory, upper secondary, university/college).
Working status was reported as employed, student, jobseeker, not gainfully employed (e.g. managing a household, retired, income support recipient not seeking work), or missing.
Sickness absence: sick leave was reported as full-time (100%) or part-time (25–75%), sickness compensation/disability pension was reported as full-time (100%) or part-time (25–75%).
Pain
Pain intensity over the last 7 days was marked on an 11-point numeric rating scale (NRS), with 0 representing “no pain” and 10 “worst pain imaginable”. Pain variation was reported by the patient describing whether the pain localization was constant or variable.
The number of pain sites was registered using 36 pre-defined anatomical areas. The patient reported the number of sites with pain on the left side of the body (n = 18) and on the right side of the body (n = 18); a total of 36 locations. These pain sites were: (1) head/face, (2) neck, (3) shoulder, (4) upper arm, (5) elbow, (6) forearm, (7) hand, (8) anterior aspect of chest, (9) lateral aspect of chest, (10) belly, (11) sexual organs, (12) upper back, (13) lower back, (14) hip/gluteal area, (15) thigh, (16) knee, (17) shank, and (18) foot.
Duration of pain was reported as the number of days since pain started and the number of days with persistent/chronic pain.
Emotional and physical functioning
The Hospital Anxiety and Depression Scale (HADS) is a measurement of anxiety (HADS-A) and depression (HADS-D) (15). The instrument consists of 7 items for anxiety and 7 items for depression. Each item can be rated from 0 to 3, whereby the respondents indicate how much it applies to them during the last week. The total scale, for each subscale of anxiety or depression, ranges between 0 and 21, a higher score indicating a worse condition. A high score indicates the need for clinical assessment for anxiety/depression. The obtained scores can be divided in 3 categories where a score of 7 or lower indicates no anxiety/depression, a score of 8–10 a mild disorder, and a score of 11 or higher is the cut-off for a possible clinically significant disorder (15).
The Functional Rating Index (FRI) measures activity and participation in relation to the International Classification of Functioning Disability and Health (ICF) (16). FRI consists of 10 questions about, for example, walking, working, lifting, pain intensity, sleep, and activities of daily living. The answers are graded on a 5-point scale. The sum of these questions is converted to a percentage, where 100% means that the patient does not perceive any function at all, while 0% means full self-rated function (16). Many patients with chronic musculoskeletal pain have chronic low back pain or chronic neck pain, and often pain in both locations. The FRI is recommended for the assessment of disability in people with multi-area spinal pain (17). Furthermore, the FRI has shown good responsiveness for patients with chronic low back pain (18) and chronic neck pain (19).
Coping
The Chronic Pain Acceptance Questionnaire (CPAQ) consists of 20 questions rated on a 7-point scale, from 0 (never true) to 6 (always true).These items can be compiled into 2 subscales: Activity Engagement (AE) consisting of 11 items (0 min to 77 max), and Pain Willingness (PW) consisting of 9 items (0 min to 63 max) (20). Activity Engagement is the degree to which the person engages in activities with pain present, while Pain Willingness is the degree to which the person refrains from attempts to avoid or control painful experiences. The items on the CPAQ are rated on a 7-point scale, from 0 (never true) to 6 (always true).
The Pain Catastrophizing Scale (PCS) consists of 13 items describing different thoughts and feelings when experiencing pain. The PCS instructions ask participants to reflect on painful experiences on a 5-point scale from 0 (not at all) to 4 (all the time). PCS yields a total score (patient’s degree of pain-related catastrophizing) from 0–52, in which 52 signifies maximal catastrophizing and 3 subscales: rumination, magnification and helplessness (21). In this study, only the total score is used.
Health-related quality of life
The Life Satisfaction Questionnaire (LiSat-11) captures the patient’s estimations of satisfaction with life as a whole (LiSat-life) as well as satisfaction in 10 specific domains (22). In this study, 2 variables were selected: satisfaction with (i) life as a whole (LiSat-life) and with (ii) vocational situation (LiSat-vocation). Each item had 6 possible answers: 1 = very dissatisfying; 2 = dissatisfying; 3 = fairly dissatisfying; 4 = fairly satisfying; 5 = satisfying; and 6 = very satisfying.
The EQ-5D European Quality of Life instrument measures HRQoL (23). The instrument consists of 2 parts: one part that measures health status in 5 dimensions (5D) and one part where the respondents evaluate their overall health status using a 100-point scale, a vertical scale where the endpoints are labelled “Best imaginable health state”’ and “’Worst imaginable health state” (EQ-VAS).
Work-related factors
Self-reported current work ability was measured with an item from the Work Ability Index (WAI) (24):”We assume that your work ability, at its best, is valued by ten points. What score would you give your current work ability?” This item was scored from 0 (completely unable to work) to 10 (best work ability). An additional question was added with the following wording “How likely is it that you will be working within the next 6 months?” Eight alternative responses were given: 1 = Extremely likely, 2 = Very likely, 3 = Quite likely, 4 = Neither likely nor unlikely, 5 = Quite unlikely, 6 = Very unlikely, 7 = Extremely unlikely, 8 = Not applicable for me (this answer was excluded from the statistical analyses).
Statistical analysis
All statistical analyses were performed using the Statistical Package for Social Sciences (version 24.0 SPSS Inc., Chicago, IL, USA). Data are reported both as means with standard deviations and median with interquartile range. Differences in patient characteristics between men and women were investigated with χ2 test, independent-samples t-test, or Mann–Whitney U test. The effects of MMRP in primary care on pain, physical and emotional functioning, coping, HRQoL and work-related factors for a group of patients with chronic pain, both as a whole and for men and women separately (primary aim) were analysed with Wilcoxon signed-rank test, paired t-test and McNemar’s test. Results with p < 0.05 (2-sided) were considered significant for all tests.
Bonferroni adjustment for multiple comparisons was made before interpreting the p-values. No imputations were used for missing values. ES were calculated for differences between women and men at baseline for all variables and for baseline vs 1-year follow-up of MMRP for the whole group of patients and for men and women respectively (primary aim). Calculations were conducted using the webpage Psychometrica (25), Cohen (1988) describes absolute ES of 0.0–0.2 as non-significant, 0.2–0.49 as small, 0.5–0.79 as medium, and ≥ 0.8 as strong. Spearman’s correlation coefficients were calculated when analysing bivariate correlations at baseline to examine risk of multicollinearity for covariates in a logistic regression model (correlation coefficient > 0.67). The correlation coefficient r was interpreted according to Taylor (26) as weak <0.35, moderate 0.36–0.67, strong 0.68–0.9, or perfect > 0.9–1.
The second aim to identify predictive factors for not being on sickness absence at follow-up was analysed by logistic regression. First, an univariate logistic regression analysis was used to analyse the association between being on no sickness absence (sick leave or disability pension) at 1-year follow-up (dependent variable) and the following variables at baseline: age, sex, educational level (compulsory/upper secondary school and university/college), self-rated ability to work (the question from WAI and the question about likelihood of working within 6 months), pain intensity during the last week, HADS-A (15), HADS-D (15), PCS (21), FRI (16), EQ-5D Index (23) CPAQ (20) and Lisat-11 (2 items were dichotomized into either satisfied 5–6 or not satisfied 1–4) (22). Variables that had a p-value < 0.1 in the univariate regression analyses were then included in a model with multiple regression analysis. The results of the logistic regression analyses are presented as an odds ratio (OR). The reliability of the OR is expressed as 95% confidence interval (95% CI). Statistical significance was set at p < 0.05 for the multiple regression analysis. Correlations between the instruments at baseline were evaluated to examine risk of multicollinearity for covariates in the logistic regression model.
Drop-out analysis
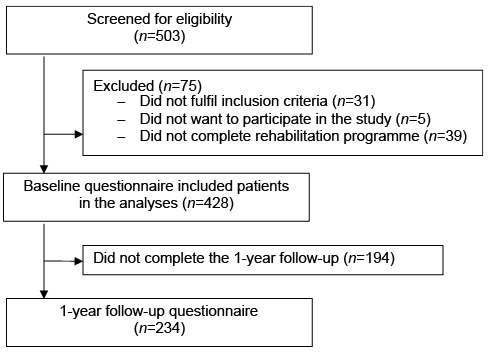
In total, 503 patients were assessed for participation in MMRP (Fig. 1). Thirty-one of these were not invited to participate because they did not fulfil all inclusion criteria, and 5 patients did not want to complete the questionnaires. Hence, 467 patients were included at baseline. Thirty-nine patients did not complete the MMRP treatment, leaving 428 patients for further analyses. A total of 234 patients (54.7%) completed the 1-year follow-up. There were no statistically significant differences in baseline characteristics between patients who did or did not complete the 1-year follow-up, except that those who completed the 1-year follow-up had a higher level of education (p = 0.004) and reported 2 points lower on pain catastrophizing (PCS: 23.1±10.8 vs 25.1±10.9, respectively, p = 0.037). Participants at the northern centres completed the 1-year follow-up more often than participants at the southern centres (n = 112 (70%) vs n = 122 (45.5%), respectively, p < 0.001).
Fig. 1. Study flow diagram.
Patient characteristics
Patient characteristics at baseline are reported in Table I. The majority of the patients were women (women, n = 200, 85.5%, men, n = 34, 14.5%). Most patients (88%) were born in Sweden. The number of years with chronic pain ranged between 1 and 40 years. Pain intensity was moderate (current: 6.0±2.0; last week: mean 6.5±1.8). Women reported a significantly higher number of pain sites than did men (15.2±8.3 vs 11.3±6.5, respectively, p = 0.003) (Table I).
Table I. Patient characteristics at baseline. Comparison between women and men
One-year follow-up after multimodal rehabilitation programmes
Significant improvements were found in all PROMs investigated, except for LiSat-vocation (Table II) for all participants as a whole. The ES for all outcomes were small (0.24–0.34). The largest ES were found for acceptance aspects according to CPAQ-AE, followed by catastrophizing (i.e. PCS).
Women improved significantly in all PROMs between baseline and 1-year follow-up. The ES were small, except for an insignificant ES (0.17) for LiSat-Life. Men only improved significantly in FRI. In men, ES were moderate (FRI), small (HADS-D, HADS-A, CPAQ-AE, CPAQ-PW, LiSat-vocation, EQ5D-Index and EQ5D-VAS), or insignificant (pain intensity during last week, PCS and EQ5D-VAS) (Table II). All ES in PROMs between baseline and 1-year follow-up were larger in women, except for ES for FRI (women ES (95% CI) –0.32 (–0.52 to –0.12) vs men –0.56 (–1.05 to –0.07), respectively) (Table II).
Table II. Change in patient-reported outcome measures between baseline and 1-year follow-up for all patients, and for women and men separately.
Sickness absence (sick leave, sickness compensation/disability pension)
At baseline, 39.7% of the patients (n = 93) were on sick leave (full-time n = 49, part-time n = 44). At follow-up, the proportion of patients on sick leave had decreased significantly (p = 0.027) to 31.6% (n = 74; full-time n = 35, part-time n = 39) (Table III). Before MMRP, 13.2% of the patients (n = 31) had sickness compensation/disability pension (full-time n = 5, part-time n = 26). At 1-year follow-up, the proportion of patients on sickness compensation/disability pension was 17.5% (n = 41) (full-time n = 13, part-time n = 28) (Table III).
Table III. Sick leave and sickness compensation/disability pension at baseline and 1-year follow-up for all patients, and for men and women separately
Correlations
Correlations between the instruments at baseline were evaluated (Table IV). The correlations were weak (0–0.30) to moderate (0.30–0.50). The strongest significant (p < 0.01) correlations were found between HADS-A and HADS-D (r = 0.686), HADS-D and LiSat-life (r = –0.607) and between FRI and EQ5D VAS (r = –0.571).
Table IV. Bivariate correlations
Univariate logistic regression and multivariate analyses
In the univariate logistic regression analysis using “being on no sickness absence” at 1-year follow-up as a dependent variable and the variables at baseline: pain intensity, FRI, self-rated work ability was significant (Table V). Variables that had a p-value < 0.1 in the univariate regression analysis were included in a multiple regression analysis (Table V). In the multiple logistic regression, only “self-rated work ability” from WAI was associated with “being on no sickness absence” at 1-year follow-up.
Table V. Univariate and multiple logistic regression between explanatory variables at baseline and probability of not being on sickness absence (dependent variable) at 1-year follow-up
In this study, the results of MMRP in primary care were evaluated using PROM and sickness absence after one year in patients with chronic pain. The results showed significant improvements in all domains (pain, physical and emotional functioning, coping, health-related quality of life, work-related factors), except for satisfaction with vocation. The proportion of patients on sick leave decreased significantly, while there was no significant difference regarding the proportion of patients on sickness compensation/disability pension.
The majority of the participants in MMRP were women, as was the case in the studies performed in specialist pain care (27, 28). This is in line with annual reports from the SQRP (12). The higher proportion of women participating in MMRP could be explained by the fact that women have a higher prevalence of chronic pain than do men (9). There may also have been a selection bias, since not all patients who undergo assessment are selected for MMRP. Some previous studies found that women were selected for MMRP more often than men (28). Qualitative interviews conducted in the same settings in primary care indicate that healthcare professionals were hesitant to refer single men to an MMRP (29).
In the Swedish healthcare system, patients with complex chronic pain are supposed to be referred to primary care MMRP, while patients with very complex chronic pain including significant psychological comorbidities are to be referred to specialist MMRP (10). The core goals of MMRP are broad and multifactorial (e.g. less psychological distress, reduced pain intensity, better coping strategies, return to work/studies and increased HRQoL) in combination with individualized goals of the patient. Some patients may improve in some variables, while others improve in other variables. Compared with our study population, patients in a study in specialist care in the same county councils were younger, but the proportions of women, country of origin and level of education were similar (28). In our study HADS-A and CPAQ-AE at baseline, before participating in MMRP were somewhat higher than in patients managed at the specialist clinics, while pain intensity, LiSat-life and CPAQ-PW at baseline were similar in both settings.
In conclusion, the differences were small between patients in primary care and in specialist care, which means that the policy-makers’ intention (10) that patients with complex or very complex chronic pain should be treated in different settings has so far not been successful. The reasons for this could be that patients with more complex pain conditions are not referred from primary care to specialist clinics, the number of specialist clinics per county council is limited, or patients do not want or are not able to travel to the specialist clinics.
In the current study, there were no differences at baseline between women and men, except that women had more pain locations. This is in line with previous studies from specialist care, which also found that women had more widespread pain (30). Molander et al. (30) studied more than 40,000 patients with chronic pain conditions who were included in the SQRP from specialist clinics, and found that, where there were sex differences, the numerical differences were small except for the spreading of pain around the body.
However, for women, all PROMs improved significantly, while for men only function improved significantly. Thus, in men, the MMRP had hardly any effect (ES less than 0.2) on pain intensity during the last week, catastrophizing, LiSat-life, and EQ5D VAS. The results of the present study are in line with the study by Pieh et al. (9), who found that women presented better effects after MMRP than men in pain-related disabilities in everyday life. Even though the present study included a small number of men, this strengthens the claim that MMRP may be more suitable for women than for men (9). However, contrary to the present study, both Pieh et al. and Koegh et al. found that men improved significantly after an MMRP (9, 30). Explanations for this could be differences in sample size, the content and length of the programme, or the time-point of measurement.
Several systematic reviews have reported that MMRP is effective for patients with chronic pain (2, 5). Although patients in this study improved significantly in all PROMs, except for satisfaction with vocation, the ES were lower than in specialist care based on national data (31, 32) and also from the same county councils for pain intensity during the last week, CPAQ-AE, CPAQ-PW, pain catastrophizing and EQ-VAS, but similar for HADS Anxiety and Depression, LiSat life, EQ5D-Index, and physical functioning for men (27).Since the ES were small, a possible explanation is that MMRP in primary care is a new intervention and specialist clinics have larger resources and more years of experience of the management of MMRP. Thus, further development of MMRP is warranted in order to improve the outcomes. Although national guidelines were published to support the assessment of patients with chronic pain with selection criteria to enhance MMRP at the appropriate level (specialist vs primary healthcare), healthcare professionals in primary care found it difficult to select patients for MMRP (29).
The teams play a central role in the coordination of MMRP. In a previous qualitative study, the importance of creating good teamwork was pointed out as a key factor for the implementation of MMRP in primary care (33). Although most studies of MMRP have been conducted in specialist care, a previous study from a primary care unit has shown promising long-term results regarding depression, social activity, physical activity and healthcare utilization after one year (34). Another study reported that improvements in pain, perceived health, quality of life and psychosomatic symptoms were maintained between 1- and 5-year follow-ups (35). Thus, our study is in accordance with these findings and emphasizes the need to offer MMRP to the large group of patients with complex chronic pain in primary care.
The rehabilitation guarantee was introduced in Sweden to reduce sick leave in patients with chronic pain. In the present study, the proportion of patients on sick leave had decreased at 1-year follow-up. This is in line with a study by Stein & Miclescu (34), who likewise found decreased sick leave in patients with chronic pain one year after MMRP in primary care in another part of Sweden. However, in our study, no difference regarding the proportion of patients on sickness compensation/disability pension was found from before MMRP to follow-up. The rehabilitation guarantee has recently been evaluated using national data from the Swedish Social Insurance Agency in an observational matched and controlled study (36). That study found that sickness absence was not reduced in patients participating in MMRP in 2009–10 compared with controls; nevertheless, MMRP was effective in reducing the risk of future disability pension. There might be several reasons for the different study results, such as different data sources, study populations and study time periods. Although the present study was conducted during the period 2012–15, at that time MMRPs were still in the phase of implementation in primary care. Since MMRP was initiated as a new rehabilitation intervention, healthcare professionals from the primary healthcare units reported both negative and positive aspects when implementing it (33). They also experienced similar difficulties in managing work ability and return to work in MMRP, as reported from other primary care units in Sweden (37). At the time of the present data collection, the MMRPs did not contain specific work-directed interventions, which have been found to be an important factor for return to work (38). In line with previous studies (39), patients’ positive expectations about work was a predictive factor for not being on sickness absence at follow-up. The patient’s own expectations indicate the importance of also including the individual patient actively in the process of return to work. MMRP has a long tradition in pain rehabilitation in specialist care, and studies have shown that MMRP improves the potential for patients with chronic pain to decrease sick leave/return to work (1). In a recent study on national data from specialist care of more than 7,000 patients with chronic pain, sick-leave benefits were increased significantly from 1 year before to the start of MMRP and decreased from the start of MMRP to 2 years after (40).
Strengths and limitations
Some limitations of the study should be noted. No control group was included and the changes between baseline and 1-year follow-up may have been caused by the effects of MMRP or may depend on other factors, such as natural course. However, patients with chronic pain have often had their condition for a long period of time, which may reduce the effect of natural course. The patients who did not complete the MMRP (39/467; 8.4%) had a lower education compared with those who did complete the MMRP, which might indicate, for example, that the programme is more suitable or accessible for patients with higher education. Not all participants answered the 1-year follow-up, which reduces the generalizability of the results. On the other hand, there were no differences between those who did or did not answer the follow-up, except that those who completed the 1-year follow-up reported somewhat lower pain catastrophizing. The MMRPs were implemented as a new intervention in primary care and the professionals were unfamiliar with a structured follow-up of patients with questionnaires, which may partly explain the differences. However, it cannot be ruled out that patients who experienced less favourable effects after MMRP were less inclined to answer the follow-up questionnaire.
The questionnaire included instruments that are widely used and have shown good validity. However, we used self-reported assessments of sickness absence, which might have impacted the validity of the sick leave information.
The number of men included was relatively low, which may have influenced the identification of differences between sexes. Therefore, besides statistically significant p-values, ES with 95% CI were also presented.
Conclusion
This study indicates that MMRP in primary care could be beneficial for patients with chronic pain and has long-term beneficial effects on pain, physical and emotional functioning, coping, and HRQoL. The ES were small, and thus further development of MMRP is warranted in order to improve the outcomes. Since the patients included had similar complexity of chronic pain, as reported by patients in specialist care, and a high proportion were on disability pension, this demonstrates that healthcare professionals in primary care were not able to follow the national guidelines. More education and training is probably needed to select and treat patients for MMRP at the primary care level. However, it should be noted that MMRP is a complex intervention, which may take time to implement in a different level of healthcare.
This study was supported by the Swedish Social Insurance Agency, the research programme REHSAM, AFA Insurance and Forsknings-ALF (county councils of Västerbotten and Östergötland).


 Click to show fullsize
Click to show fullsize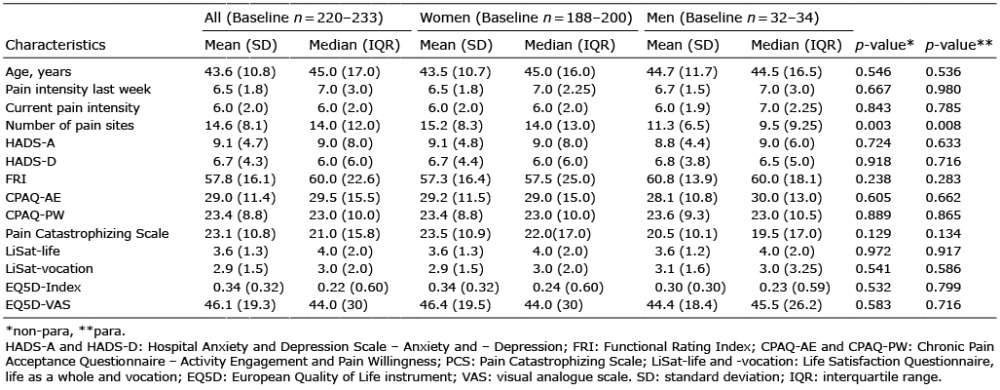 Click to show fullsize
Click to show fullsize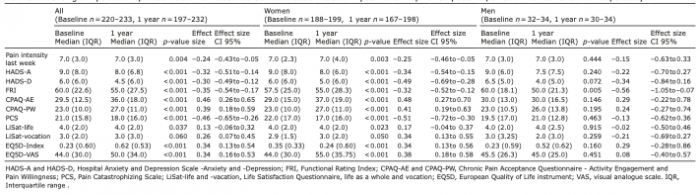 Click to show fullsize
Click to show fullsize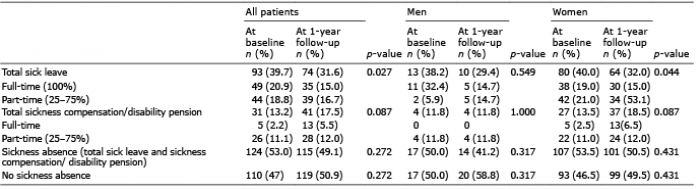 Click to show fullsize
Click to show fullsize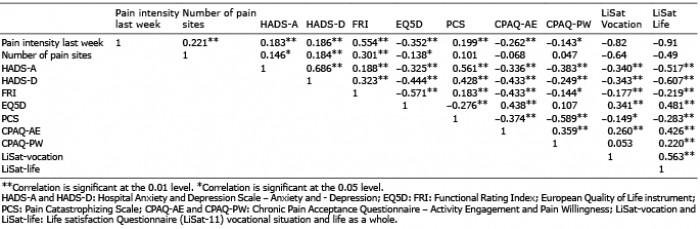 Click to show fullsize
Click to show fullsize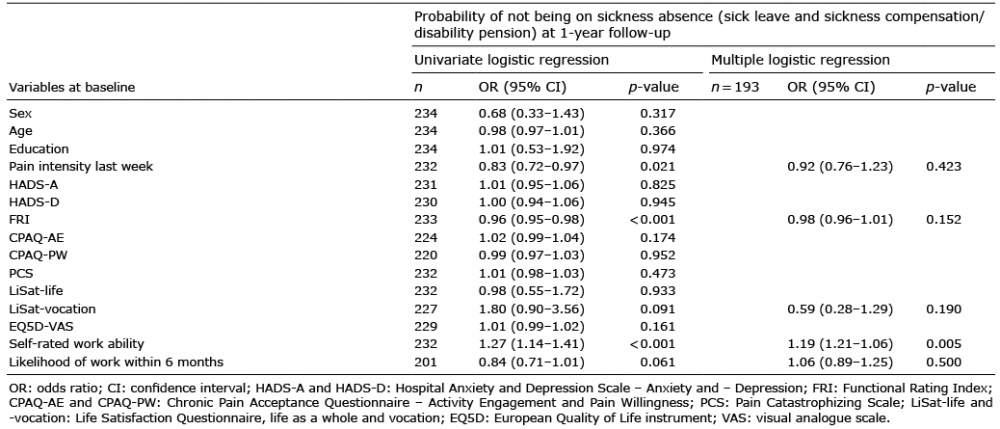 Click to show fullsize
Click to show fullsize